Rest
Sleep as a biological prerequisite for longevity and repair
For many people, wellness begins the morning after a good night of sleep.
The body feels lighter. Mood is steadier. Cravings are quieter. Workouts feel more productive. Stress becomes more manageable. When sleep improves, people often say they feel “more like themselves.”
That shift isn’t just psychological. It’s biological.
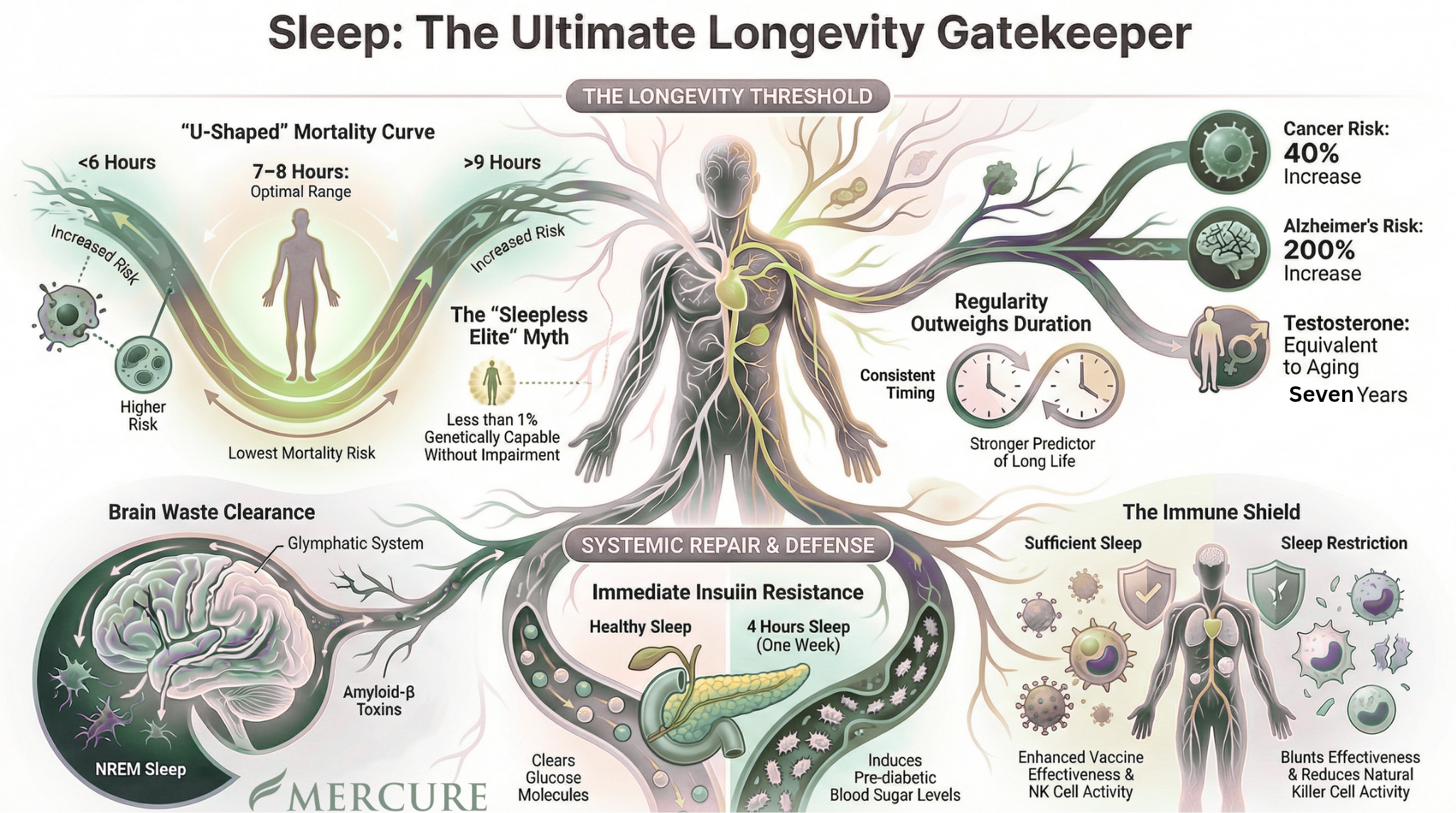
Sleep is not passive downtime. It’s the body’s primary nightly window for repair—when the brain clears metabolic waste, the endocrine system recalibrates, and the immune system shifts its inflammatory tone. When sleep becomes irregular, fragmented, or insufficient, longevity suffers—often before any diagnosis appears.
Sleep Is a Biological Input
Sleep is frequently treated as a lifestyle variable: something we “get” when we’re done being productive.
In the medical literature, sleep functions more like a biological input that shapes aging across multiple systems. Large-scale cohort data show a U-shaped relationship between sleep duration and health outcomes: both short sleep (often ≤6 hours) and long sleep (often ≥8–9 hours) are associated with increased mortality risk, compared with the most consistently favorable range near 7–8 hours.¹²³⁴⁵
Even more striking: sleep regularity may predict mortality more strongly than duration. In large prospective cohorts, more regular sleep patterns are associated with meaningfully lower all-cause mortality risk—even after adjusting for how long someone sleeps.⁶⁷
The takeaway is simple and clinically useful:
Longevity is not just about “more sleep.” It’s about stable, reparative sleep—consistently.
The Nervous System Bridge: Why Sleep Gets “Stuck”
Sleep is one of the clearest places the nervous system reveals its state.
When the nervous system is in a threat posture—hyperarousal, stress overload, persistent vigilance—sleep onset and sleep maintenance become harder. Even if someone is exhausted, the system may resist downshifting.
This matters because the biological consequences of poor sleep accumulate through predictable pathways:
Stress physiology: Sleep restriction disrupts circadian cortisol rhythm and increases overall cortisol exposure, with particularly notable elevations later in the day.⁹
Anabolic–catabolic balance: Sleep loss reduces testosterone secretion across multiple measures while cortisol trends upward, contributing to an anabolic-catabolic imbalance.⁶⁷
Inflammation signaling: Acute sleep loss may not immediately elevate circulating CRP or IL-6, but it activates upstream inflammatory pathways at the genomic level, and multiple nights of partial sleep deprivation reliably increase circulating inflammatory proteins.¹²³⁴
Immune function: Sleep restriction impairs immune response (including reduced vaccine antibody response) and increases vulnerability to infections.¹²¹³¹⁴
Sleep isn’t simply about discipline. It’s about capacity.
“Sleep as a Longevity Gatekeeper”
The U-shaped mortality curve (sleep regularity + brain + metabolic/hormonal + inflammation/immune)
From Feeling Better to Progressing
A single good night of sleep can create an immediate improvement in mood, performance, and cravings. But longevity depends on something deeper:
sleep architecture and consistency.
Sleep supports memory consolidation through features of non-REM sleep (slow oscillations and spindles) and REM sleep.¹⁰ When sleep is disrupted, cognitive performance, attention, executive function, and short-term memory decline—especially functions dependent on the prefrontal cortex.¹⁰
Longer-term patterns matter even more. Disturbed sleep is associated with markers of impaired brain health and neurodegenerative risk. Both short and long sleep durations have been associated with worse brain structure metrics and cognitive outcomes.⁸⁹ Sleep disorders are recognized as important contributors to adverse brain health outcomes including cognitive decline and Alzheimer disease.¹⁰
Sleep, then, is not only how you feel tomorrow.
It’s how your brain ages over years.
Common Misunderstandings About Sleep and Longevity
“If I’m in bed longer, I’m recovering.”
Time in bed is not the same as reparative sleep. Long sleep duration is often associated with increased cardiovascular and stroke mortality in observational research.⁴ The clinical point is not to restrict sleep intentionally, but to recognize that persistent long sleep can be a signal—sleep fragmentation, inflammation, depression, or underlying disease burden.
“I can catch up on weekends.”
Recovery sleep helps, but it does not reliably restore everything. Some immune and inflammatory parameters remain impaired even after recovery sleep, suggesting that chronic sleep restriction is not fully neutralized by brief rebound periods.¹⁹
“Sleep is passive.”
Sleep is one of the most metabolically active “repair states” the body enters. When sleep is disrupted, downstream systems begin to shift—metabolism, inflammation, hormones, cognition.
Ways to Strengthen Rest Capacity
These aren’t hacks or rules. Think of them as inputs that make sleep easier for the body to receive—especially when stress, travel, or high demands are present.
1) Build Regularity First (Before You Chase Perfect Hours)
Sleep regularity may predict mortality risk more strongly than sleep duration itself.⁶⁷
Rather than aiming for “more sleep” every night, anchor a consistent wake time most days of the week. Regularity stabilizes circadian signaling across the brain and peripheral tissues.
2) Protect a Predictable Downshift Window
If your nervous system runs “hot,” sleep often fails at the downshift. A 30–60 minute transition period helps the body recognize that rest is safe. Keep it simple and repeatable:
dim lighting
lower stimulation
warm shower or rinse
slow breathing (longer exhales)
Consistency matters more than intensity.
3) Treat Sleep Like Metabolic Hygiene
Sleep restriction impairs insulin sensitivity—even without weight change—and can shift metabolic function measurably within weeks.²³⁴
If cravings, appetite, or energy regulation feel “off” during periods of poor sleep, interpret it as physiology—not a character flaw. Support the system first, then expect behavior to follow.
Small, predictable signals of support are often more regulating than dramatic effort.
Portal Support: Rest as a Physiological Environment
Some people benefit from pairing behavioral change with environments that reliably support nervous system downshifting.
Two Portal modalities map cleanly to the physiology of rest:
Sauna + Cold Plunge: Heat exposure and cold exposure can support stress tolerance and autonomic recalibration when used thoughtfully. If you want to learn more about The Portal’s sauna and cold plunge experience, you can view it here: https://www.theportal.house/sauna-coldplunge.
Shiftwave: Nervous system entrainment may support downshifting out of hyperarousal, especially in individuals who struggle to “turn off” at night.
These are not sleep treatments—but they can be sleep-supportive inputs when the nervous system needs help accessing a rest state.
A Clinical Next Step: When Sleep Needs Medical Support
If sleep disruption persists despite consistent behavioral support, it may reflect an underlying physiological driver that benefits from evaluation—particularly when symptoms include:
persistent fatigue despite time in bed
waking frequently
early-morning awakenings with anxiety
low libido, mood changes, or reduced recovery
metabolic markers shifting (weight gain, glucose dysregulation)
Sleep affects hormonal and metabolic systems in measurable ways. Sleep restriction induces insulin resistance,²³⁴ disrupts cortisol rhythm,⁹ and shifts testosterone-cortisol balance.⁶⁷ Sleep architecture (especially slow-wave sleep) is also linked to androgen secretion.⁸
For individuals focused on longevity, sleep is often the highest-leverage place to investigate medically.
If you want to explore medical optimization strategies—including labs, hormonal drivers, and sleep-related physiology—you can learn more here:
👉 Hormone Optimization & Functional Medicine Services
Support doesn’t have to be guesswork. It can be evaluated, measured, and strengthened.
References
Yang L, et al. J Epidemiol Community Health. 2021. doi:10.1136/jech-2020-215314.
Ungvari Z, et al. GeroScience. 2025. doi:10.1007/s11357-025-01592-y.
Saint-Maurice PF, et al. Sleep. 2024. doi:10.1093/sleep/zsad312.
Jike M, et al. Sleep Med Rev. 2018. doi:10.1016/j.smrv.2017.06.011.
Gao C, et al. Front Med. 2021. doi:10.3389/fmed.2021.813943.
Windred DP, et al. Sleep. 2024. doi:10.1093/sleep/zsad253.
Chung J, et al. J Sleep Res. 2024. doi:10.1111/jsr.14048.
Namsrai T, et al. Sci Rep. 2023. doi:10.1038/s41598-023-27913-9.
Stolicyn A, et al. Sleep. 2024. doi:10.1093/sleep/zsad274.
Gottesman RF, et al. Stroke. 2024. doi:10.1161/STR.0000000000000453.
Winer JR, et al. JAMA Neurol. 2021. doi:10.1001/jamaneurol.2021.2876.
Rao MN, et al. J Clin Endocrinol Metab. 2015. doi:10.1210/jc.2014-3911.
Sondrup N, et al. Sleep Med Rev. 2022. doi:10.101594.
Zuraikat FM, et al. Diabetes Care. 2024. doi:10.2337/dc23-1156.
Liu PY, Reddy RT. Rev Endocr Metab Disord. 2022. doi:10.1007/s11154-022-09755-4.
Liu PY, et al. Sleep. 2020. doi:10.1093/sleep/zsaa008.
Ukraintseva YV, et al. Sleep Med. 2018. doi:10.1016/j.sleep.2018.04.012.
Guyon A, et al. J Clin Endocrinol Metab. 2014. doi:10.1210/jc.2013-4254.
Irwin MR, et al. Biol Psychiatry. 2016. doi:10.1016/j.biopsych.2015.05.014.
Ballesio A, et al. J Sleep Res. 2025. doi:10.1111/jsr.70099.
Irwin MR, et al. Arch Intern Med. 2006. doi:10.1001/archinte.166.16.1756.
Spiegel K, et al. Curr Biol. 2023. doi:10.1016/j.cub.2023.02.017.
Prather AA, et al. Sleep. 2012. doi:10.5665/sleep.1990.
Martínez-Albert E, et al. Phil Trans R Soc B. 2025. doi:10.1098/rstb.2023.0472.
Faraut B, et al. Sleep Med Rev. 2012. doi:10.1016/j.smrv.2011.05.001.